Herpes Triggers Amyloid—Could This Virus Fuel Alzheimer’s?
Quick Links
Aβ is generally considered a rogue peptide, but recent research is building a case that it may have a secret identity as an antimicrobial superhero. Confronted with an unwelcome bacteria or fungus, the peptide quickly forms amyloid fibrils that ensnare the invader. Is this response to pathogens relevant to the development of Alzheimer’s disease? The idea is controversial, but new data from two complementary papers make it more plausible. First, a gene-expression network analysis led by Joel Dudley at Mount Sinai, New York, reported human herpesviruses 6 and 7 to be more abundant in AD than control brains, and linked these viruses to upregulation of many genes involved in amyloidosis (Jun 2018 news). Now, researchers led by Rudolph Tanzi and Robert Moir at Massachusetts General Hospital, Charlestown, offer a mechanism to explain this association. In the July 11 Neuron, they report that herpes simplex virus 1 (HSV-1) and human herpesvirus activate Aβ’s superpower, just as bacteria and fungi do. The viruses sparked rapid amyloidosis in mouse and cellular models of AD; this response protected neurons from infection and helped AD mice live longer after a viral challenge. The work is available on bioRχiv, and Neuron has lifted its embargo on the manuscript.
- Aβ42 protects neurons and mice from infection by herpes viruses.
- The peptide binds viral particles and rapidly fibrillizes, forming sticky nets.
- As a result, viral infections bring on amyloidosis in AD models within 48 hours.
The amyloid hypothesis of AD holds that amyloidosis kicks off downstream pathologies, such as tau tangles and neuroinflammation, which lead to dementia.
“When you take the two papers together, they provide a complete picture of how herpes virus may accelerate and enhance the progression of AD,” Moir told Alzforum. “Viral seeding of plaque can be regarded as a prequel to the amyloid hypothesis,” he and Tanzi wrote to Alzforum (full comment below).
Moir acknowledged that it remains uncertain whether the virus by itself can initiate the disease. Even if it does, infection likely represents but one possible trigger for Alzheimer’s pathology, he stressed. Other cases may be purely genetic, caused by overproduction or poor clearance of the peptide. Howard Federoff at the University of California, Irvine, said the data bolster the theory that Alzheimer’s disease is actually many diseases. “There may be disparate triggers that lie upstream of a common pathway of Aβ induction and fibrillization,” Federoff suggested.
Others called the data exciting. “The concept that Aβ fibrils can act as pathogen nets—ensnaring and then trapping herpesviruses—is remarkable and unanticipated,” Terrence Town at the University of Southern California, Los Angeles, wrote to Alzforum (full comment below). “This paper properly highlights the anti-infective nature of Aβ amyloid,” wrote Brian Balin, Philadelphia College of Osteopathic Medicine, Pennsylvania, and Alan Hudson, Wayne State University School of Medicine, Detroit (full comment below).

Viruses Provoke Amyloidosis.
The subiculum of young 5xFAD mice (left) is normally free of plaques (blue), but 48 hours after injection of HSV-1 (red), plaques encase viral particles (right, overlay appears purple). [Courtesy of Neuron, Eimer et al.]
The idea that infections might stimulate AD has been around since at least the 1990s, championed by researchers such as Balin and Ruth Itzhaki at the University of Manchester, U.K. (e.g., July 2004 webinar). It received a boost when Tanzi, Moir, and colleagues proposed that Aβ functions as an antimicrobial peptide, shutting down bacterial and fungal replication in vitro (Apr 2009 conference news; Mar 2010 news).
The MGH researchers subsequently showed that the peptide formed sticky nets that ensnared pathogenic yeast and bacteria in animal and cell culture models, helping the cell or host organism to survive (May 2016 news). Alas, few other labs jumped in to study the topic, though some researchers have reported analogous findings in Parkinson’s, turning up evidence that α-synuclein, too, functions as an antimicrobial (May 2017 news; Jul 2017 news; Apr 2018 news).
Yeast and bacteria are not that common in human brain. Herpes viruses are. Some studies claim that nearly everyone carries these viruses, usually since early childhood, and they often reach the central nervous system (Jamieson et al., 1991). Herpes viruses are found in 90 percent of amyloid plaques, and active infections have been linked to AD risk (Wozniak et al., 2009; Letenneur et al., 2008; Feb 2011 webinar). “Herpes virus is the No. 1 pathogen associated with AD,” Moir noted.
To test Aβ’s response to these pathogens, first author William Eimer injected a lethal dose of HSV1 into the hippocampi of five- to six-week-old 5xFAD mice and controls. At this age, plaques have not yet formed, but Aβ levels are high. The AD mice survived longer, with half of them still alive after two days, when nearly all controls had already succumbed to the infection.
Moreover, in the AD mice, amyloid plaques popped up within 48 hours of virus injection, surrounding viral particles (see image above). Plaques did not form in sham-injected 5xFAD mice, nor in wild-type controls injected with virus. In a separate experiment, the researchers injected young 5xFAD mice with non-lethal doses of HSV1 and saw advanced amyloidosis in their cortices three weeks later. The data suggest that a low-level viral infection in the brain can still accelerate amyloid formation, the authors noted.
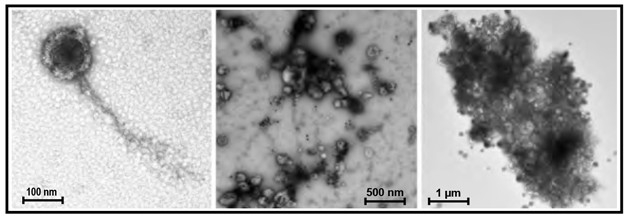
Snare that Virus. Aβ42 rapidly cocoons viral particles, forming fibrils after 15 minutes (left), nets after 30 (middle), and impenetrable clumps after two hours (right). [Courtesy of Neuron, Eimer et al.]
How might viruses do this? Eimer and colleagues report that Aβ42 oligomers bind to HSV1 through glycoprotein B, a component of the viral envelope that helps viruses enter host cells. Antibodies to this glycoprotein competitively inhibited Aβ binding, but did not entirely eliminate it, suggesting the peptide may bind other moieties as well. After Aβ42 oligomers bound glycoprotein B, they immediately began to fibrillize. Within minutes, viral particles in vitro sported long fibril tails (see image above). Moir noted that this accoutrement would prevent viruses from penetrating cells, effectively neutralizing the infection. Fibrillization itself continues, however. Within an hour, viral particles were linked by a sticky net of Aβ strands. After two hours, gobs of amyloid completely sequestered the viruses and began to break down viral envelopes, destroying the microbes.
While most people have HSV1 in their peripheral nervous system, the virus does not always get into the brain. Human herpesvirus 6 (HHV-6) is much more common there, with some estimates putting it at close to 100 percent prevalence. The authors could not test this virus in mice because mice resist HHV-6 infection due to genetic differences in a cellular receptor between mice and humans. Instead, the authors added HHV-6A to three-week-old, three-dimensional neural cell cultures that model aspects of Alzheimer’s pathology (Oct 2014 news). These cultures normally do not form amyloid plaques before six weeks, but 48 hours after addition of HHV-6A, they were peppered with fibrillar deposits. As with HSV-1, Aβ42 bound to glycoprotein B in HHV-6A’s viral envelope and rapidly fibrillized.
Charlotte Warren-Gash at the London School of Hygiene and Tropical Medicine considers the case for Aβ acting as an antimicrobial peptide convincing, but cautioned the findings may have little relevance for AD. She noted that only a small proportion of people experience HSV-1 outbreaks. “During latency—the commonest state—there is very little viral gene expression. … Reactivating herpes viruses may be just one of a range of factors that can accelerate some part of the aging process, but disentangling their effects from those of other environmental, social, and lifestyle factors remains a formidable challenge,” she wrote to Alzforum (full comment below).
Moir agrees that viruses are likely to play a role in only a subset of AD cases. People have differing susceptibilities to viral infection, with some never experiencing outbreaks, and others having them regularly. A combination of genetic and environmental factors may affect how active viral infections are in a given person, he suggested. In particular, the ApoE4 allele seems to supercharge the immune response, improving survival in pathogen-rich environments early in life (Vasunilashorn et al., 2011; Fujioka et al., 2013; Gale et al., 2014; van Exel et al., 2017). Late in life, this aggressiveness may become a liability if the brain overreacts to recurrent viral outbreaks by producing too much amyloid, Moir speculated.
“Immune responses are a double-edged sword. Amyloidosis may be analogous to a fever—a protective host response that can get out of hand and cause damage,” he suggested. This excess of amyloid can lead to inflammation, Moir noted. Other research suggests that this neuroinflammation, not plaques or tangles, is responsible for neuronal death and dementia (Perez-Nievas et al., 2013).
Federoff said an interaction between ApoE4 and the immune response would not surprise him. In previous research on human ApoE knock-in mice infected with HSV-1, he found that those carrying the E4 allele had trouble suppressing viral activity, with their infections less likely to enter latency (Miller and Federoff, 2008). It is unclear how this finding relates to ApoE4’s proinflammatory effects.
As further evidence of a link between viruses and AD, Moir points to a Taiwanese population study of more than 33,000 adults, which found that recent HSV-1 infections conferred a 2.5-fold increased risk of developing dementia. This risk dropped back to baseline for those treated with antiviral medication (Tzeng et al., 2018). “That’s nice evidence that antiviral drugs are effective in reducing your risk for AD,” Moir said. The challenge will be to identify the people who might benefit from such treatment, he added. Federoff wondered whether Dudley’s recent transcriptome data might provide potential biomarkers for active CNS viral infections.
Another new paper, currently available as a preprint on bioRχiv, adds genetic evidence for HSV-1 playing a role in AD. Researchers led by Robert Graham at Genentech, South San Francisco, identified the functional variant linked to a protective GWAS hit as being a missense mutation in the paired immunoglobulin-like type 2 receptor alpha (PILRA). PILRA is a microglia receptor that dampens inflammation.
To examine the effects of the G78R missense variant, first author Nisha Rathore transfected the variant and the normal protein into a kidney cell line. Rathore and colleagues found that G78R weakened binding to several endogenous ligands. Because the virus HSV-1 uses PILRA to enter cells, the authors tested this as well, and found the missense variant reduced its binding by half.
Graham and colleagues wondered if the G78R variant might protect carriers from viral infection. They isolated monocyte-derived macrophages from five people homozygous for the variant, and five homozygous for the normal gene. When the cells were exposed to HSV-1, those carrying the variant resisted infection, accumulating five- to 10-fold less HSV-1 DNA than controls. The results suggest that resistance to HSV-1 infection could help protect against Alzheimer’s, the authors noted.
While several studies now strengthen the case for viral infections as a risk factor for AD, Moir sees little utility in treating people who already have the disease with antivirals. “Aβ is like the match that sets fire to the underbrush, sparking tau tangles, which then start a forest fire of neuroinflammation,” he said.—Madolyn Bowman Rogers
References
News Citations
- Aberrant Networks in Alzheimer’s Tied to Herpes Viruses
- Prague: Aβ Rehabilitated as an Antimicrobial Protein?
- Paper Alert: Aβ’s Day Job—Slayer of Microbes?
- Like a Tiny Spider-Man, Aβ May Fight Infection by Cocooning Microbes
- Olfactory System Model Explores Antimicrobial Role for α-Synuclein
- Put ’Em Up: Does α-Synuclein Help Fight Microbes in the Gut?
- Do Immune Responses Promote, or Prevent, Parkinson’s Disease?
- Alzheimer’s in a Dish? Aβ Stokes Tau Pathology in Third Dimension
Webinar Citations
Paper Citations
- Jamieson GA, Maitland NJ, Craske J, Wilcock GK, Itzhaki RF. Detection of herpes simplex virus type 1 DNA sequences in normal and Alzheimer's disease brain using polymerase chain reaction. Biochem Soc Trans. 1991 Apr;19(2):122S. PubMed.
- Wozniak MA, Mee AP, Itzhaki RF. Herpes simplex virus type 1 DNA is located within Alzheimer's disease amyloid plaques. J Pathol. 2009 Jan;217(1):131-8. PubMed.
- Letenneur L, Pérès K, Fleury H, Garrigue I, Barberger-Gateau P, Helmer C, Orgogozo JM, Gauthier S, Dartigues JF. Seropositivity to herpes simplex virus antibodies and risk of Alzheimer's disease: a population-based cohort study. PLoS One. 2008;3(11):e3637. PubMed.
- Vasunilashorn S, Finch CE, Crimmins EM, Vikman SA, Stieglitz J, Gurven M, Kaplan H, Allayee H. Inflammatory gene variants in the Tsimane, an indigenous Bolivian population with a high infectious load. Biodemography Soc Biol. 2011;57(1):33-52. PubMed.
- Fujioka H, Phelix CF, Friedland RP, Zhu X, Perry EA, Castellani RJ, Perry G. Apolipoprotein E4 prevents growth of malaria at the intraerythrocyte stage: implications for differences in racial susceptibility to Alzheimer's disease. J Health Care Poor Underserved. 2013 Nov;24(4 Suppl):70-8. PubMed.
- Gale SC, Gao L, Mikacenic C, Coyle SM, Rafaels N, Murray Dudenkov T, Madenspacher JH, Draper DW, Ge W, Aloor JJ, Azzam KM, Lai L, Blackshear PJ, Calvano SE, Barnes KC, Lowry SF, Corbett S, Wurfel MM, Fessler MB. APOε4 is associated with enhanced in vivo innate immune responses in human subjects. J Allergy Clin Immunol. 2014 Jul;134(1):127-34. Epub 2014 Mar 18 PubMed.
- van Exel E, Koopman JJ, Bodegom DV, Meij JJ, Knijff P, Ziem JB, Finch CE, Westendorp RG. Effect of APOE ε4 allele on survival and fertility in an adverse environment. PLoS One. 2017;12(7):e0179497. Epub 2017 Jul 6 PubMed.
- Perez-Nievas BG, Stein TD, Tai HC, Dols-Icardo O, Scotton TC, Barroeta-Espar I, Fernandez-Carballo L, de Munain EL, Perez J, Marquie M, Serrano-Pozo A, Frosch MP, Lowe V, Parisi JE, Petersen RC, Ikonomovic MD, López OL, Klunk W, Hyman BT, Gómez-Isla T. Dissecting phenotypic traits linked to human resilience to Alzheimer's pathology. Brain. 2013 Aug;136(Pt 8):2510-26. PubMed.
- Miller RM, Federoff HJ. Isoform-specific effects of ApoE on HSV immediate early gene expression and establishment of latency. Neurobiol Aging. 2008 Jan;29(1):71-7. PubMed.
- Tzeng NS, Chung CH, Lin FH, Chiang CP, Yeh CB, Huang SY, Lu RB, Chang HA, Kao YC, Yeh HW, Chiang WS, Chou YC, Tsao CH, Wu YF, Chien WC. Anti-herpetic Medications and Reduced Risk of Dementia in Patients with Herpes Simplex Virus Infections-a Nationwide, Population-Based Cohort Study in Taiwan. Neurotherapeutics. 2018 Apr;15(2):417-429. PubMed.
Other Citations
External Citations
Further Reading
Primary Papers
- Eimer WA, Vijaya Kumar DK, Navalpur Shanmugam NK, Rodriguez AS, Mitchell T, Washicosky KJ, György B, Breakefield XO, Tanzi RE, Moir RD. Alzheimer's Disease-Associated β-Amyloid Is Rapidly Seeded by Herpesviridae to Protect against Brain Infection. Neuron. 2018 Jul 11;99(1):56-63.e3. PubMed.
Annotate
To make an annotation you must Login or Register.
Comments
Massachusetts General Hospital
Massachusetts General Hospital & Harvard Medical School
Our study, taken together with the Readhead et al. findings, suggest a new model for amyloidogenesis in which chronic elevated viral replication may directly promote Aβ deposition in AD brain. In this model, the activation of herpes viruses serves to rapidly “seed” amyloid plaque formation.
Along these lines, we can now consider other microbes—viral, bacterial, or fungal—that may likewise rapidly seed amyloid. Moreover, we can consider other possible “seeds” for amyloid deposition beyond microbes, e.g., particulate air pollution, heavy metals. In addition, most early onset familial AD mutations increase the ratio of Aβ42:Aβ40, which also promotes seeding of amyloid plaques. Some data also suggest APOE4 seeds plaques better than APOE3.
While some have argued that AD genetic findings argue against an infectious etiology, the genetic findings can be interpreted to put forward a common thread—enhanced seeding of Aβ. For example, in the context of microbial seeding of plaques as an innate immune response to defend host cells from infection, early onset familial AD mutations can be considered as constitutive activators of seeding (via increased Aβ42:Aβ40 ratio) resulting in early onset dementia, without the involvement or need for microbial seeding. One can also argue that in the early history of humans, early onset familial Alzheimer’s mutations may have conferred a selective advantage against childhood or early adult brain infections.
Interestingly, a missense mutation in the PILRA gene which yields genome-wide significant protection against AD has been reported to impair cellular infection by HSV1 (Rathore et al., 2018). Other genes encoding viral receptors have also been associated with AD, e.g. ITGB3 (Loehlein et al., 2017).
We believe the combined findings in Eimer et al. and Readhead et al. present an important new chapter in understanding AD etiology and pathogenesis, whereby elevated levels of herpes viruses and, perhaps, other microbes in the brain, may initiate or exacerbate AD pathology.
The emerging role for microbes in AD also suggest antivirals and antimicrobials may be considered for early therapeutic intervention. Along these lines, these two new studies are timely given the recent report that antiherpetic medications in a Taiwan population may reduce AD risk for patients with herpes CNS infection by 2.5-fold (Tzeng et al., 2018).
In closing, we hope our data, along with the Readhead et al. findings and other recent studies, will lead to a broader consideration of the possible role of infection in AD and a greater concerted effort by the research community at large to explore this line of investigation.
References:
Rathore N, Ramani SR, Pantua H, Payandeh J, Bhangale T, Wuster A, Kapoor M, Sun Y, Kapadia SB, Gonzalez L, Zarrin AA, Goate A, Hansen DV, Behrens TW, Graham RR. Paired Immunoglobulin-like Type 2 Receptor Alpha G78R variant alters ligand binding and confers protection to Alzheimer's disease. PLoS Genet. 2018 Nov;14(11):e1007427. Epub 2018 Nov 2 PubMed.
Loehlein Fier H, Prokopenko D, Hecker J, Cho MH, Silverman EK, Weiss ST, Tanzi RE, Lange C. On the association analysis of genome-sequencing data: A spatial clustering approach for partitioning the entire genome into nonoverlapping windows. Genet Epidemiol. 2017 May;41(4):332-340. Epub 2017 Mar 20 PubMed.
Tzeng NS, Chung CH, Lin FH, Chiang CP, Yeh CB, Huang SY, Lu RB, Chang HA, Kao YC, Yeh HW, Chiang WS, Chou YC, Tsao CH, Wu YF, Chien WC. Anti-herpetic Medications and Reduced Risk of Dementia in Patients with Herpes Simplex Virus Infections-a Nationwide, Population-Based Cohort Study in Taiwan. Neurotherapeutics. 2018 Apr;15(2):417-429. PubMed.
University of Southern California
The authors have devised an extraordinarily creative hypothesis. The concept that Aβ fibrils can act as pathogen nets—ensnaring and then trapping herpesviruses—is remarkable and unanticipated.
This direct link between Aβ and immunity is compelling; casting fibrils and plaques as physiologically relevant in stark contrast to their much-maligned roles in AD pathobiology. The evolutionary game of hare and fox between herpesviruses and Aβ is fascinating.
Philadelphia College of Osteopathic Medicine
Wayne State University School of Medicine
This paper properly highlights the anti-infective AMP nature of Aβ amyloid. These data, with previous work from this and other laboratories, provide a rationale as to why amyloid would accumulate in the Alzheimer’s brain, as well as in brain in other neurodegenerative conditions. However, as the authors clearly state, their report and the associated paper by Readhead et al. do not demonstrate causality, although they do provide strong evidence for correlation of viral infection with AD. What is not addressed in these reports is accumulation of amyloid in a significant number of individuals in whom cognitive change is not apparent, and what that may mean. Herpesviridae are ubiquitous human pathogens with prevalence approaching 100 percent (Campadelli-Fiume et al., 1999; Jamieson et al., 1991). This being the case, many control individuals also have Herpesviridae in the brain but no apparent neurocognitive changes. Does amyloid accumulate in the brain wherever the virus may be harbored, and if so, does this imply that specific brain regions must be infected in order to cause neurocognitive change? Further, other factors including specific genetic profiles and various environmental insults may be required to initiate and propagate neurodegeneration.
Certainly other infectious agents may be included in a multifactorial scenario for initiation of neurodegeneration; such a situation seems to us to be more direct in triggering pathogenesis than Herpesviridae alone, although different herpetic viruses such as HSV1 may be more involved with initial triggering (Itzhaki and Lathe, 2018). In this regard, generalized infection in the brain may not cause the problem but may exacerbate the problem following other, more specific insults. Specific infection of selectively vulnerable sites in the body may be required to trigger neuroinflammation and/or amyloid production, processing, and deposition engendering subsequent neuropathogenesis. What has been intriguing for decades is the selective vulnerability of regions of the brain in which AD first manifests.
The lateral entorhinal cortex and hippocampus appear to be the early sites of damage in a majority of AD individuals. The input from the olfactory system into the lateral entorhinal cortex implicates olfaction in this process, and the olfactory neuroepithelium in the upper respiratory system implicates the airborne environment as a source of insult. This specific pathway is of significant interest since infectious agents, pollution, trauma, etc. can result in damage to the very regions of the brain in which AD begins. The blood-brain barrier also has been implicated, although intracellular infection or insult in the olfactory system will bypass the blood-brain barrier and is more direct and specific than the blood-brain barrier to the brain areas demonstrating early pathology.
Thus, the possibility exists that more than one pathway, and indeed more than one particular insult, is involved in triggering or causing the initial changes in the brain leading to neurocognitive deficit. In our work on Chlamydia pneumoniae involvement in AD, we realize that this ubiquitous intracellular bacterial pathogen may use both the olfactory system and the blood to enter the brain. We have demonstrated evidence for both (Balin et al., 1998; Gerard et al., 2006; Little et al., 2004, 2014). Chlamydia pneumoniae is a respiratory pathogen, and access to the olfactory portions of the brain via nostrils and lungs facilitates its uptake directly into a nerve pathway. As a blood-borne pathogen, Chlamydia pneumoniae infects monocytes and lymphocytes surveilling lung tissues, which brings to bear the issue of “neurotropism” and “monocyte and/or lymphotropism” as mechanisms by which numerous organisms may gain entry to the brain. Both pathways appear to be involved—Chlamydia pneumoniae appears to use both. The question remains, though, as to what are primary versus secondary infections. In either case, a polymicrobial infection appears to be immediately relevant, as numerous reports of several different organisms associated with AD have been published in the past two decades (Itzhaki et al, 2016).
The overall importance of the current work on Herpesviridae and its apparent association with AD supports a paradigm shift in thinking about AD neuropathogenesis. With the focus having been on amyloid and tau for the past 30-plus years, the time has come to accept that answers to the AD puzzle, and possibly other neurodegenerative conditions as well, does not reside solely in the pathology, but in the route to that pathology, for which infectious agents provide biologically and pathologically relevant solutions.
References:
Campadelli-Fiume G, Mirandola P, Menotti L. Human herpesvirus 6: An emerging pathogen. Emerg Infect Dis. 1999 May-Jun;5(3):353-66. PubMed.
Jamieson GA, Maitland NJ, Wilcock GK, Craske J, Itzhaki RF. Latent herpes simplex virus type 1 in normal and Alzheimer's disease brains. J Med Virol. 1991 Apr;33(4):224-7. PubMed.
Itzhaki RF, Lathe R. Herpes Viruses and Senile Dementia: First Population Evidence for a Causal Link. J Alzheimers Dis. 2018;64(2):363-366. PubMed.
Balin BJ, Gérard HC, Arking EJ, Appelt DM, Branigan PJ, Abrams JT, Whittum-Hudson JA, Hudson AP. Identification and localization of Chlamydia pneumoniae in the Alzheimer's brain. Med Microbiol Immunol. 1998 Jun;187(1):23-42. PubMed.
Gérard HC, Dreses-Werringloer U, Wildt KS, Deka S, Oszust C, Balin BJ, Frey WH, Bordayo EZ, Whittum-Hudson JA, Hudson AP. Chlamydophila (Chlamydia) pneumoniae in the Alzheimer's brain. FEMS Immunol Med Microbiol. 2006 Dec;48(3):355-66. PubMed.
Little CS, Hammond CJ, MacIntyre A, Balin BJ, Appelt DM. Chlamydia pneumoniae induces Alzheimer-like amyloid plaques in brains of BALB/c mice. Neurobiol Aging. 2004 Apr;25(4):419-29. PubMed.
Little CS, Joyce TA, Hammond CJ, Matta H, Cahn D, Appelt DM, Balin BJ. Detection of bacterial antigens and Alzheimer's disease-like pathology in the central nervous system of BALB/c mice following intranasal infection with a laboratory isolate of Chlamydia pneumoniae. Front Aging Neurosci. 2014;6:304. Epub 2014 Dec 5 PubMed.
Itzhaki RF, Lathe R, Balin BJ, Ball MJ, Bearer EL, Braak H, Bullido MJ, Carter C, Clerici M, Cosby SL, Del Tredici K, Field H, Fulop T, Grassi C, Griffin WS, Haas J, Hudson AP, Kamer AR, Kell DB, Licastro F, Letenneur L, Lövheim H, Mancuso R, Miklossy J, Otth C, Palamara AT, Perry G, Preston C, Pretorius E, Strandberg T, Tabet N, Taylor-Robinson SD, Whittum-Hudson JA. Microbes and Alzheimer's Disease. J Alzheimers Dis. 2016;51(4):979-84. PubMed.
London School of Hygiene and Tropical Medicine
This paper offers convincing evidence that active HSV-1 and HHV-6 infections in 5XFAD mice and human neural cell cultures induce Aβ fibrillization, adding further weight to the argument that Aβ counts antimicrobial peptide activity among its pleiotropic effects.
But does it support the infection aetiology hypothesis for Alzheimer’s disease? Human herpesviruses are not as ubiquitous as the authors suggest: In an older U.K. population, around 64 percent have ever been infected with HSV-1. While infection persists lifelong, only a relatively small proportion of people reactivate HSV-1 sufficient to cause clinically apparent disease.
The immune system and the virus exist in a delicate equilibrium, but during latency—the commonest state—there is very little viral gene expression and, presumably, very little innate immune system activation. HSV-1 reactivations have been shown to decrease in frequency with age, believed to be due to depletion of viral genome copy number.
If HSV-1 were to reactivate in the human brain, Aβ deposition may well occur. But given the disconnect between neuropathology and cognition, especially at older ages, the clinical importance of this finding is unclear. Reactivating herpesviruses may be just one of a range of factors that can accelerate some part of the aging process, but disentangling their effects from those of other environmental, social, and lifestyle factors remains a formidable challenge.
ASU-Banner, Neurodegenerative Disease Research Center
This paper provides compelling support for the antimicrobial protection hypothesis of Alzheimer's disease. It's not yet clear whether herpesviridae represent a causative factor in Alzheimer's disease etiology. Even so, the discovery that rapid (<15 minutes) Aβ fibrillization is mediated by Aβ42 binding to conserved carbohydrates in the envelope glycoprotein-B of HSV-1, and HHV-6 offers a specific and parsimonious mechanism that links microbial activity within the brain to β-amyloidosis.
We recently reported a persistently increased abundance of HHV-6A, HHV-7, and HSV-1 within postmortem brain tissue samples collected from individuals with Alzheimer's. Through multi-omic network modelling, we observed that HHV-6A induced the expression of many regulators of APP metabolism, e.g. APBB2, APPBP2, BIN1, BACE1, CLU, PICALM, and PSEN1.
In the context of insights provided by Eimer et al., our data could suggest that these networks reflect the transcriptomic underpinnings of a sustained, virally induced β-amyloidosis response.
Does anyone think it's significant that seven of 12 genes shown to be upregulated in cells harboring latent HSV-1 are also upregulated in Alzheimer's patients brains? (See lists of each below).
Eight Genes Upregulated in Alzheimer's Brain tissue:
PLAUR Plasminogen activator, urokinase receptor (Walker et al., 2002)
CA2 Carbonic anhydrase 2 (Jang et al., 2010; Sultana et al., 2010)
MMP3 Matrix metallopeptidase 3 (Horstmann et al., 2010)
EGR1 Early growth response (Gómez Ravetti et al., 2010)
PDE1A Phosphodiesterase 1A, calmodulin-dependent (Sun et al., 2014)
CRH Corticotropin releasing hormone (Meynen et al., 2017; Raadsheer, et al., 1995)
ADAMTS1 A disintegrin-like and metallopeptidse (reprolysin type)with thrombospondin type 1 motif (Miguel et al., 2005)
Cathepsin D, likely equivalent to CTSJ cathepsin J of rat observed with HSV (Mufson et al., 2002; Cataldo et al., 1995; Haas and Sparks, 1996)
Out of 12 observed upregulated in HSV latency (Danaher, 2008):
CTSJ Cathepsin J in rat (likely equivalent to Human Cathepsin D)
MMP10 Matrix metallopeptidase 10
PLAUR Plasminogen activator, urokinase receptor
CA2 Carbonic anhydrase 2
MMP3 Matrix metallopeptidase 3
EGR1 Early growth response
ST3GAL4 ST3 beta-galactoside alpha-2,3-sialyltransferase 4
MMP13 Matrix metallopeptidase 13
PDE1A Phosphodiesterase 1A, calmodulin-dependent
NEU2 Neuraminidase 2
CRH Corticotropin releasing hormone
ADAMTS1 A disintegrin-like and metallopeptidse (reprolysin type) with thrombospondin type 1 motif
References:
Walker DG, Lue LF, Beach TG. Increased expression of the urokinase plasminogen-activator receptor in amyloid beta peptide-treated human brain microglia and in AD brains. Brain Res. 2002 Feb 1;926(1-2):69-79. PubMed.
Jang BG, Yun SM, Ahn K, Song JH, Jo SA, Kim YY, Kim DK, Park MH, Han C, Koh YH. Plasma carbonic anhydrase II protein is elevated in Alzheimer's disease. J Alzheimers Dis. 2010;21(3):939-45. PubMed.
Sultana R, Perluigi M, Newman SF, Pierce WM, Cini C, Coccia R, Butterfield DA. Redox proteomic analysis of carbonylated brain proteins in mild cognitive impairment and early Alzheimer's disease. Antioxid Redox Signal. 2010 Mar;12(3):327-36. PubMed.
Horstmann S, Budig L, Gardner H, Koziol J, Deuschle M, Schilling C, Wagner S. Matrix metalloproteinases in peripheral blood and cerebrospinal fluid in patients with Alzheimer's disease. Int Psychogeriatr. 2010 Sep;22(6):966-72. Epub 2010 Jun 18 PubMed.
Gómez Ravetti M, Rosso OA, Berretta R, Moscato P. Uncovering molecular biomarkers that correlate cognitive decline with the changes of hippocampus' gene expression profiles in Alzheimer's disease. PLoS One. 2010;5(4):e10153. PubMed.
Sun J, Song F, Wang J, Han G, Bai Z, Xie B, Feng X, Jia J, Duan Y, Lei H. Hidden risk genes with high-order intragenic epistasis in Alzheimer's disease. J Alzheimers Dis. 2014;41(4):1039-56. PubMed.
Meynen G, Unmehopa UA, Hofman MA, Swaab DF, Hoogendijk WJ. Relation between corticotropin-releasing hormone neuron number in the hypothalamic paraventricular nucleus and depressive state in Alzheimer's disease. Neuroendocrinology. 2007;85(1):37-44. PubMed.
Raadsheer FC, van Heerikhuize JJ, Lucassen PJ, Hoogendijk WJ, Tilders FJ, Swaab DF. Corticotropin-releasing hormone mRNA levels in the paraventricular nucleus of patients with Alzheimer's disease and depression. Am J Psychiatry. 1995 Sep;152(9):1372-6. PubMed.
Luk KC, Covell DJ, Kehm VM, Zhang B, Song IY, Byrne MD, Pitkin RM, Decker SC, Trojanowski JQ, Lee VM. Molecular and Biological Compatibility with Host Alpha-Synuclein Influences Fibril Pathogenicity. Cell Rep. 2016 Sep 20;16(12):3373-87. PubMed.
Miguel RF, Pollak A, Lubec G. Metalloproteinase ADAMTS-1 but not ADAMTS-5 is manifold overexpressed in neurodegenerative disorders as Down syndrome, Alzheimer's and Pick's disease. Brain Res Mol Brain Res. 2005 Jan 5;133(1):1-5. PubMed.
Mufson EJ, Counts SE, Ginsberg SD. Gene expression profiles of cholinergic nucleus basalis neurons in Alzheimer's disease. Neurochem Res. 2002 Oct;27(10):1035-48. PubMed.
Cataldo AM, Barnett JL, Berman SA, Li J, Quarless S, Bursztajn S, Lippa C, Nixon RA. Gene expression and cellular content of cathepsin D in Alzheimer's disease brain: evidence for early up-regulation of the endosomal-lysosomal system. Neuron. 1995 Mar;14(3):671-80. PubMed.
Haas U, Sparks DL. Cortical cathepsin D activity and immunolocalization in Alzheimer disease, critical coronary artery disease, and aging. Mol Chem Neuropathol. 1996 Sep;29(1):1-14. PubMed.
Danaher RJ, McGarrell BS, Stromberg AJ, Miller CS. Herpes simplex virus type 1 modulates cellular gene expression during quiescent infection of neuronal cells. Arch Virol. 2008;153(7):1335-45. Epub 2008 Jun 12 PubMed.
Ottawa Hospital Research Institute
This paper by Eimer et al. and also Readhead et al., 2018, are both really exciting.
I speculate that in years to come, people will remember them as the beginning of a new era in AD research. In the field of late-onset disorders of the brain, we have long neglected to pay more attention to the possible interactions between a host’s genome and his/her exposure history (exposome), including ubiquitously present, viral pathogens. These interactions underlie complex disease development.
They also contribute to the vast majority of late-onset diseases in humans.
Exploring Alzheimer’s disease and the process of β-amyloidosis in the context of a host responding to the presence of microbial structures, such as Herpesviridae, or related signaling—rather than doing so exclusively from a neuroscientific angle without an exposome component—is what allowed the two teams to make these stimulating and likely game-changing observations.
In my view, these insights will not only enrich the field of sporadic, late-onset AD, but also research into typical, late-onset Parkinson’s, which historically is 10 years behind AD research. The two papers will invigorate our quest for etiological clues in many neurodegenerative disorders, and undoubtedly for better-informed therapeutic approaches in the future.
Congratulations are due to both teams.
References:
Readhead B, Haure-Mirande JV, Funk CC, Richards MA, Shannon P, Haroutunian V, Sano M, Liang WS, Beckmann ND, Price ND, Reiman EM, Schadt EE, Ehrlich ME, Gandy S, Dudley JT. Multiscale Analysis of Independent Alzheimer's Cohorts Finds Disruption of Molecular, Genetic, and Clinical Networks by Human Herpesvirus. Neuron. 2018 Jul 11;99(1):64-82.e7. Epub 2018 Jun 21 PubMed.
Universities of Manchester and Oxford
It's good to see the excitement about the role of herpes viruses in AD elicited by the studies of Readhead et al. and Eimer et al., and good to know that the discovery, 28 years ago, of HSV1 DNA in elderly human brains by simple PCR (Jamieson et al., 1991) has now been confirmed. What a pleasing contrast the current response is to the venom—or the dismissals—that greeted that first paper and most subsequent ones from my lab and the labs of many others. These included the first paper to show that HSV1 causes Aβ accumulation (Wozniak et al., 2007), and earlier, that HSV1 in brains of APOE-e4 carriers is a major risk for AD, and APOE-e4 a major risk for cold sores (Itzhaki et al., 1997).
However, Aβ's role has now undergone a striking volte face: Eimer et al. present further evidence that Aβ, produced by HSV1 and HHV6 infection, is not simply a toxic end product but instead an antimicrobial peptide—a cell protector when in a fibrillar oligomeric state, acting by entrapping the offending microbe. In the case of herpes viruses, the authors show that Aβ42 oligomers inhibit HSV1 infection in vitro and protect 5XFAD transgenic mice from the acute viral disease of herpes encephalitis. The mechanism involves Aβ42 binding to and agglutinating HSV1 and HHV6, probably via the viral envelope glycoprotein B; this induces fibrillization, and thence, the formation of an insoluble fibril/virus agglutinate.
The authors suggest that viral seeding of Aβ in the brain is rapid and dramatic, “various conformers of Aβ acting as innate intra-CNS mediators of resistance that protect the brain from herpesviridae infection.” They consider that as viruses minimize extracellular exposure, rapid Aβ fibrillization is probably advantageous for ensnaring HSV1 and HHV6 before the viruses can adhere to host cells.
In AD, Eimer et al. suggest that the protective antimicrobial pathways are overactivated by infection, thus conferring a risk of AD-related pathogenic β-amyloidosis, and that the change of Aβ from protective to neuropathological might reflect pathogen virulence and persistence, host genetics, or environmental factors. It would be most interesting to know how that change occurs, and also how APOE-e4 fits in the picture, especially as it has been suggested that it might compete with HSV1 for attachment to cell receptors. This hypothesis is supported by the fact that APOE genotype determines an individual's response to HSV1 and to microbes of very diverse types (Itzhaki and Wozniak, 2009).
Interestingly, there are two much earlier papers relevant to that of Eimer et al. The first, by Robinson and Bishop (2002), proposed that Aβ is a general chelator and flocculant of potentially toxic agents that are dissolved in the extracellular fluid, ranging from metal ions to bacteria and viruses present in the extracellular fluid. This followed a suggestion by Berthon (2000) that Aβ may exert a protective function against the iron-induced oxidative stress associated with neurological diseases. The “bioflocculant hypothesis” posited that Aβ “is normally produced to bind neurotoxic solutes or microbes, and that the precipitation of Aβ into plaques may be an efficient means of presenting these toxins to phagocytes.” Robinson and Bishop concluded that if Aβ deposition represented a physiological response to injury, then therapeutic treatments aimed at reducing the availability of Aβ might hasten the disease process and associated cognitive decline in AD: a prescient thought. Unfortunately, in the usual response to novel ideas, their suggestion was either derided or ignored.
Puzzlingly, the other study (Wojtowicz et al., 2002) reported a positive effect of Aβ on HSV1 infection, although in this case it was the shorter peptide Aβ1-40, and synthetic fibrils were used. It was found that the enhancement of infection occurred at the stage of virus attachment or entry into the cell. The peptide concentration was similar to that used by Eimer et al., so whether the contrast with the latter authors' results reflects differences in the Aβ peptides used, or differences in their preparation, is unknown.
Lastly, there is an intriguing current study (Ezzat et al., 2018) concerned with the viral corona. This is a layer of host factors which surround the virus similar to those on nanoparticles, and dependent on the microenvironment. This corona very probably influences virus-host interactions, viral infectivity, and immune cell activation. HSV1, and also respiratory syncytial virus (RSV), which were shown to act as nanosurface catalysts for the aggregation of amyloid peptides, including Aβ. More information about the structure and function of the corona, and how it fits into the picture of Aβ's transformation from benign to toxic, will surely be of great interest.
References:
Readhead B, Haure-Mirande JV, Funk CC, Richards MA, Shannon P, Haroutunian V, Sano M, Liang WS, Beckmann ND, Price ND, Reiman EM, Schadt EE, Ehrlich ME, Gandy S, Dudley JT. Multiscale Analysis of Independent Alzheimer's Cohorts Finds Disruption of Molecular, Genetic, and Clinical Networks by Human Herpesvirus. Neuron. 2018 Jul 11;99(1):64-82.e7. Epub 2018 Jun 21 PubMed.
Eimer WA, Vijaya Kumar DK, Navalpur Shanmugam NK, Rodriguez AS, Mitchell T, Washicosky KJ, György B, Breakefield XO, Tanzi RE, Moir RD. Alzheimer's Disease-Associated β-Amyloid Is Rapidly Seeded by Herpesviridae to Protect against Brain Infection. Neuron. 2018 Jul 11;99(1):56-63.e3. PubMed.
Jamieson GA, Maitland NJ, Wilcock GK, Craske J, Itzhaki RF. Latent herpes simplex virus type 1 in normal and Alzheimer's disease brains. J Med Virol. 1991 Apr;33(4):224-7. PubMed.
Wozniak MA, Itzhaki RF, Shipley SJ, Dobson CB. Herpes simplex virus infection causes cellular beta-amyloid accumulation and secretase upregulation. Neurosci Lett. 2007 Dec 18;429(2-3):95-100. PubMed.
Itzhaki RF, Lin WR, Shang D, Wilcock GK, Faragher B, Jamieson GA. Herpes simplex virus type 1 in brain and risk of Alzheimer's disease. Lancet. 1997 Jan 25;349(9047):241-4. PubMed.
Itzhaki RF, Wozniak MA. Apolipoprotein E: Microbial Friend or Foe?. In: Apoprotein Research, Eds: LR Penfield and RT Nelson 2009. Nova Science Publishers Inc., New York.
Robinson SR, Bishop GM. Abeta as a bioflocculant: implications for the amyloid hypothesis of Alzheimer's disease. Neurobiol Aging. 2002 Nov-Dec;23(6):1051-72. PubMed.
Berthon G. Does human betaA4 exert a protective function against oxidative stress in Alzheimer's disease?. Med Hypotheses. 2000 Apr;54(4):672-7. PubMed.
Wojtowicz WM, Farzan M, Joyal JL, Carter K, Babcock GJ, Israel DI, Sodroski J, Mirzabekov T. Stimulation of enveloped virus infection by beta-amyloid fibrils. J Biol Chem. 2002 Sep 20;277(38):35019-24. PubMed.
Ezzat K, Pernemalm M, Pålsson S, Roberts TC, Järver P, Dondalska A, Bestas B, Sobkowiak MJ, Levänen B, Sköld M, Thompson EA, Saher O, Kari OK, Lajunen T, Sverremark Ekström E, Nilsson C, Ishchenko Y, Malm T, Wood MJ, Power UF, Masich S, Lindén A, Sandberg JK, Lehtiö J, Spetz AL, El Andaloussi S. The viral protein corona directs viral pathogenesis and amyloid aggregation. Nat Commun. 2019 May 27;10(1):2331. PubMed.
Umeå University
Umeå University
We welcome this very interesting and important contribution by Eimer and coworkers. The study shows that amyloid-β is an important antimicrobial peptide against herpes simplex virus (HSV) infections in vivo, and that HSV infection seeds amyloid plaque formation. In 2015, we published two epidemiological studies showing increased risk of later Alzheimer’s disease development for people having antibodies towards HSV (Lovheim et al., 2015; Lovheim et al., 2014). The study by Eimer and coworkers provides a likely explanation for these associations.
This and other studies over the last years have established that an important physiological role for Aβ is as an antimicrobial peptide, providing a strong link between CNS infections and Alzheimer’s disease. It also means that the hypothesis of Alzheimer’s disease being a result of infection is fully compatible with the central role of Aβ. HSV1 has emerged as the most important candidate pathogen associated with Alzheimer’s disease, with studies from many independent groups using very different methods supporting that association. The importance of this manuscript is that it provides evidence of a direct connection between the Aβ reaction in vivo and this specific pathogen.
The most exciting thing about the connection between HSV and Alzheimer’s disease is that HSV infection can be held back with already approved and effective antiviral drugs such as valaciclovir. Whether such treatment can affect basic Alzheimer’s disease processes remains to be investigated. We have recently started a first pilot clinical trial treating persons with early Alzheimer’s disease with valaciclovir, and measuring effects of the treatment on Alzheimer’s disease biomarkers in cerebrospinal fluid. Participant recruitment is currently ongoing and the first results can be expected in 2019.
References:
Lövheim H, Gilthorpe J, Adolfsson R, Nilsson LG, Elgh F. Reactivated herpes simplex infection increases the risk of Alzheimer's disease. Alzheimers Dement. 2015 Jun;11(6):593-9. Epub 2014 Jul 17 PubMed.
Lövheim H, Gilthorpe J, Johansson A, Eriksson S, Hallmans G, Elgh F. Herpes simplex infection and the risk of Alzheimer's disease-A nested case-control study. Alzheimers Dement. 2014 Oct 7; PubMed.
Warwick University (alumnus)
I have long suspected the cause of AD to be viral, characterizing it as a "shingles of the brain," and that amyloid production is likely protective rather than toxic. These results link the two ideas: amyloid fibrils are a defense against viral attack. I think the amyloid hypothesis is simply wrong. My hunch is neurons are destroyed by viral attack, and the mechanism is fatal disruption of transport.
Make a Comment
To make a comment you must login or register.