More Needed Than Ever, Brain Banks Are Modernizing But Face Funding Crunch
( 3 Articles Available, 0 Articles Pending )
Banked brain tissue enables crucial advances in the understanding and treatment of degenerative disorders. As appreciation of the many different variants of neurodegenerative disease is growing, well-preserved tissue is in more demand than ever. Are the brain banks up to the task? Modern banks are harmonizing protocols, combining their inventories in online listings, and maintaining databases of detailed longitudinal data. At the same time, these institutions face funding shortfalls that threaten continued progress. Read Madolyn Bowman Rogers' series for the latest news, and browse Alzforum’s listing of banks around the world. [Photograph provided by the Netherlands Brain Bank, Netherlands Institute for Neuroscience, Amsterdam.]
Innovate, Then Stagnate? Brain Banks Improve Access But Are Now in Peril
To some, brain banks are creepy places that store and catalog frozen pieces of dead people’s central nervous systems. To neurodegenerative disease researchers, they provide a crucial service. Investigators need diseased tissue to glean insights into mechanisms and possible treatments. Pathology reports nail diagnoses, allowing clinicians to better manage new patients. Just last week, proceedings at the NIA’s Alzheimer’s Disease Research Summit 2015 were shot through with comments about the need for excellent brain banking in the field. Alas, all has not been well with brain banks of late. Just when researchers require more high-quality, well-characterized brain tissue than ever to parse the earliest stages of disease, these institutions face funding shortfalls that threaten their existence. Most brain banks store insufficient material to meet demand, and merely combining samples from several banks is not a solution because processing and storage systems are not standardized.
To overcome these shortcomings, modern banks are evolving. Globally, their curators are embracing the idea of big data and have created large databases of merged brain bank inventories. In turn, neuropathologists are grappling with the challenges of managing large data sets so information can be cataloged, stored, analyzed, and shared. They are also beginning to standardize protocols for processing tissue. These changes already are making it easier for researchers to find and match samples from different banks. Alzforum maintains a listing of consortia and individual brain banks around the world.
This series summarizes the strides that brain banks have made and the problems that remain. Part 1 covers the history, purpose, and funding of brain banks, Part 2 describes networks now in use across the world, and Part 3 delineates resources for specific diseases such as Alzheimer’s and Parkinson’s—some quite powerful and arguably underused.
Processing Brain Donations.
Once lifted gently from a donor’s skull, half the brain is cut into thick coronal slices for flash-freezing. The other half is fixed in formalin [Images courtesy of the Wisconsin Brain Donor Program.]
Brains Undergird Big Findings
Brain banks have been around for decades, often associated with medical centers and universities. Many are small, have only a few dedicated personnel, and share morgue space, offices, and neuropathology services with hospitals. For example, the brain bank supported by the Wisconsin Alzheimer’s Disease Research Center in Madison is a typical mid-size bank with more than 300 donor samples. It employs three full-time staff (a manager, coordinator, and pathologist), and rents space in a secure research wing of the William S. Middleton Veterans Memorial Hospital. Tissue, blood, and cerebrospinal fluid samples are housed in several freezer units. Here, bright pink slabs of brain rest in labeled boxes, safely maintained at 80 degrees below zero Celsius behind frosty inner doors. The brain bank uses facilities at the new University of Wisconsin Hospital’s morgue, a brightly lit room where gleaming stainless-steel tables and weighing scales provide cold contrast to the human organs pickling in formalin in jars on the shelves.
Given their modest size, brain banks have wielded enormous impact. Not only do their autopsies confirm diagnoses and help train residents and medical students, but the study of stored tissue has produced breakthroughs in neurodegenerative disease research. “The discovery of the amyloid β fragment was first made in postmortem frozen tissue,” pointed out Nigel Cairns, a neuropathologist at Washington University in St. Louis, Missouri (Glenner and Wong, 1984). Likewise, banked tissue helped identify α-synuclein in Parkinson’s disease, tau in frontotemporal dementia (FTD), and TDP-43 in amyotrophic lateral sclerosis (ALS). More recently, researchers used genetic material from banked cases of FTD to identify the C9ORF72 gene, a major cause of ALS and FTD (Sep 2011 news).
With that, have all the important discoveries been made? Au contraire, neurologists say. As they analyze banked brains, neurologists continue to discover previously unrecognized diseases, such as senile complex tauopathy (Kovacs et al., 2011), and subtypes of known diseases, for example a variant of FTD caused by a mutation in the PRKAR1B gene (Wong et al., 2014). Importantly, understanding variants of Alzheimer’s, such as the hippocampal-sparing form, or evolving concepts, like primary age-related tauopathy, aka PART, would be unthinkable without good material from brain banks for researchers to study (Murray et al., 2011; Crary et al., 2014).
As molecular brain imaging is advancing rapidly with the discovery of PET tracers for tau, microglial activation, and amyloid beta, autopsy tissue is essential to validate what the tracers are actually binding and how to use them for differential diagnosis. If anything, brain imagers and neuropathologists are tightening their dialogue. For example, two of the three invited keynote lectures at the Human Amyloid Imaging meeting last month in Miami Beach, Florida, were by neuropathologists who are drawing heavily on brain banks to advance research on tauopathies (play lectures at HAI; Feb 2015 conference news).
Brain banks can expose problems with current diagnostic standards. For example, neuropathologist Thomas Beach at Banner Sun Health Research Institute, Sun City, Arizona, compared clinical and pathological diagnoses on banked brains from 919 dementia patients. Even though the patients had been seen at specialty clinics, their AD diagnoses were correct in only about 70 percent of cases (Beach et al., 2012). The reliability of clinical diagnoses directly affects the success of trials, said Walter Schulz-Schaeffer, a neuropathologist at the University of Göttingen, Germany. “For each 10 percent of diagnoses that are incorrect, we have to double the study group to get significant results,” he told Alzforum.
Findings facilitated by brain banks can quite directly improve patient treatment. For example, autoimmune encephalitis, a disorder in which the immune system attacks the brain, causes memory and speech problems and is often mistaken for dementia, said Annemieke Rozemuller, a neuropathologist at the Netherlands Brain Bank in Amsterdam. The disease can be treated with anti-inflammatory drugs if it’s caught early, but if misdiagnosed and untreated, it can lead to lasting brain damage. By studying banked brain tissue and associated clinical data from people with autoimmune encephalitis, Rozemuller was able to pinpoint biomarker and brain scan changes that mark the condition. She then trained neurologists how to recognize the disorder, leading to faster and more effective treatment for many patients.
Cold Storage.
Untreated brain slices are kept at 80 degrees below zero Celsius. Researchers extract proteins and DNA from these samples for biochemical and genetic experiments.
[Photograph courtesy of the Netherlands Brain Bank, Netherlands Institute for Neuroscience, Amsterdam.]
Pathology studies also point toward new therapeutic strategies. Schulz-Schaeffer wanted to know how α-synuclein damages neurons in Parkinson’s disease. By studying donated brain tissue from patients, he found that more than 90 percent of α-synuclein aggregates occurred not in Lewy bodies, but in microaggregates at individual presynaptic terminals. At these synapses, dendritic spines retracted, breaking the connection between nerve cells (see Feb 2007 news story on Kramer and Schulz-Schaeffer, 2007). The finding suggests that Parkinson’s could be better treated in the long run by rescuing synapses rather than by simply replacing neurotransmitters, Schulz-Schaeffer said.
Each such finding sets off new research. The present drugs for treating Alzheimer’s were identified based on studies of postmortem human brain tissue more than 30 years ago, Beach noted in a commentary in the Journal of Alzheimer's Disease. However, since that time, funding for studies that use human brain tissue has dropped to one-tenth of what it once was, Beach writes. He even blames this waning support for the “Valley of Death,” the field’s much-deplored inability to carry basic research findings forward to new approved treatments (Beach, 2013). “It may be because of this funding decline that we are not discovering new therapeutic approaches at the rate we used to,” Beach wrote to Alzforum.
As Money Dries Up, Future Looms Uncertain
Neuropathologists around the world told Alzforum that funding represents the biggest current challenge for brain banks. European banks in particular are suffering, as grants from the European Commission have run out. Banks now are expected to support themselves by charging user fees, supplemented with local support from hospitals and universities and grants from neuroscience institutes. “We are struggling to pay for the basics now,” said Schulz-Schaeffer. Likewise, government support for Australian banks ended last year. Banks in the United States still enjoy some public funding, but it does not cover everything, and directors must tap multiple other monetary streams to make up for the shortfall. Increasingly, banks are eyeing collaborations with the deeper pockets of industry, Rozemuller said. This move brings its own caveats, as brain banks strive to keep their materials freely available to all researchers (Graeber, 2008).
The funding shortage curtails brain banks’ ability to acquire new tissue. An autopsy can run to $10,000, including the costs of transporting the body, dissecting and processing the brain, conducting complex neuropathologic assessment, and storing material, Cairns told Alzforum. Ironically, many banks are forced to turn away brain donations just as researchers need more material. “At the moment in time when science is exploding, the funding is contracting,” said Thomas Montine at the University of Washington, Seattle. “We have built these precious resources with taxpayer money over the last 30 years, but it takes time and money to maintain what we have, and even more to grow them.”
This means that researchers who request tissue have to modify their experiments to use fewer samples than they had planned, or investigate a different brain area because some, like the hippocampus, are both small and in high demand. “There is not enough tissue to meet all of the research requests. We could be doing more definitive experiments if we had greater resources,” Montine noted.
Brain banks face other difficulties as well. Most banks need more brain donations from normal controls of all ages, as well as from minorities and from people at preclinical stages of disease. Simply encouraging more donations from the public will not solve the problem, however. That’s because the most valuable samples come from people who have participated in longitudinal studies of aging or memory. Such donations are a precious capstone on extensive cognitive and clinical data that allow researchers to correlate pathology with the symptoms and biomarker changes the person had during life. Therefore brain banks prioritize these autopsies over “walk-ins,” and many willing donors have trouble finding a brain bank that will take them. People interested in donating can join a longitudinal study, but few such studies exist because they are expensive.
Last but not least, lack of money for training has led to a dearth of young neuropathologists in Europe. “We grow grayer and grayer, and nobody is coming to replace us,” said Rozemuller. In the last 50 years, the number of neuropathologists on staff at the Netherlands Brain Bank has dropped from 65 to about 15, she added.—Madolyn Rogers
Europe Leads the Way Toward Standardization and Brain Bank Networks
This story was updated on February 24, 2015.
No one in the field of neurodegeneration research disputes the central importance of brain banks, but that does not mean there are no complaints about them. For one, the quality of banked tissue varies widely. It depends on how soon the brain is removed after a person dies, and how scientists then handle the tissue. Because some research programs, such as those studying RNA or DNA, require well-preserved samples, neuroscientists in Europe decided to improve and harmonize protocols for processing and neuropathological diagnosis. To try to develop a gold standard, in 2001 leading European neuropathologists founded a consortium called BrainNet Europe. This organization established recommended protocols and ethical guidelines for European brain banks, although member banks are not compelled to follow them. Nineteen European banks have joined the consortium, according to Thomas Arzberger at Ludwig-Maximilian University in Munich, who manages its scientific projects.
Thin Slices.
Fixed brain sections embedded in paraffin are sliced into wafer-thin sections on a microtome.
[Photo courtesy of the Netherlands Brain Bank.]
BrainNet Europe provides a single point of contact for anyone wishing to use its member banks. Researchers from around the world can request tissue online, provided their project has ethics approval. The BrainNet office forwards the request to individual banks. As is the case with nearly all banks, requesters pay processing and shipping costs. In addition to its tissue collections, BrainNet Europe maintains a database of associated clinical findings from its roughly 2,000 cases, which include neurodegenerative and psychiatric disorders as well as controls. However, access to this database is restricted to members of the consortium.
The United Kingdom maintains a national consortium as well. The UK Brain Banks Network comprises 10 banks that together store tissue from more than 10,000 brains. Member banks have adopted standard protocols for processing tissue. Researchers from around the world can search an online database and submit tissue requests. The network fulfills more than 300 requests per year, noted director Seth Love at the University of Bristol. The U.K. network also emphasizes the collection of tissue from healthy controls. It runs a longitudinal study on 3,000 volunteers, more than half of whom do not have a neurologic diagnosis. Volunteers donate their brains after death. Some of the U.K. member banks are also members of BrainNet Europe.
On the other side of the globe, in Australia, neuroscience researchers addressed the problem of finding enough tissue by forming the Australian Brain Bank Network (ABBN) in 2004. Australia has six small, regional banks that store a few hundred brains each. They were not always able to meet research requests, and shipping expenses made going overseas for samples impractical. ABBN combines the inventories of all member banks into a single online catalog of more than 2,500 brains from adult donors who had a variety of diseases. Most cases include clinical records, and a few have longitudinal data.
Slide Preparation.
A technician transfers brain sections to slides for staining.
[Photo courtesy of Netherlands Brain Bank.]
As with BrainNet Europe, researchers from any country can request tissue from ABBN online. ABBN has fulfilled more than 1,000 tissue requests over the past 10 years, and sent tissue abroad to South Asian countries, said ABBN director Catriona McLean at Alfred Hospital in Melbourne. The organization also encourages future donations through its website. People willing to give their brain to research can sign up with the network; about 3,500 have done so already, McLean said.
New Initiative Provides Single Portal to U.S. Brain Banks
Until recently, the United States did not have a similar general-purpose brain-bank network (though it has been developing a rich collection of Alzheimer’s brains in particular; see Part 3 of this series). In September 2013, three institutes at NIH—the National Institute of Neurological Disorders and Stroke (NINDS), the National Institute of Mental Health (NIMH), and the National Institute of Child Health and Human Development (NICHD)—launched a joint initiative called the NeuroBioBank. This effort links together six large repositories through a common Web portal. These comprise the Harvard Brain Tissue Resource Center at McLean Hospital, Belmont, Massachusetts; the Human Brain and Spinal Fluid Resource Center at the University of California, Los Angeles; the University of Miami Brain Endowment Bank; the Mount Sinai Brain and Tissue Repository in New York City; the University of Maryland Brain and Tissue Bank, Baltimore; and the Brain Tissue Donation Program at the University of Pittsburgh. Other banks may join the collaboration, noted Michelle Freund at NIMH, who leads the effort along with Anna Taylor at NINDS.
Adding Color. A technician stains slides to reveal different pathological features. [Image courtesy of Nigel Cairns, Washington University, St. Louis.]
The NeuroBioBank project aims to improve researchers’ access to a variety of brain tissue, Freund said. Many banks specialize in one or two diseases, so in the past researchers could not always find the samples they needed from their local bank. To use the NeuroBioBank, scientists submit an online tissue request; the six centers review it and indicate whether they have materials that match. Also in 2013, the centers adopted the same protocols for collecting, processing, and storing brain samples. Clinical records associated with each sample follow a standard format and will be collated into a single database. In the year since the project began, the centers have collected 500 new brains using the standard protocols, Freund said. In the near future, these tissues will be listed in a catalog researchers can browse. Older, archived materials at each center, altogether totaling thousands of brains, may not appear in the catalog, but will remain available through tissue requests, noted Deborah Mash, who directs the University of Miami bank.
The NeuroBioBank supports the collection of tissues from people who had a broad range of conditions, including neurodegenerative diseases such as Parkinson’s, Huntington’s, and ALS; neurodevelopmental disorders like autism and Fragile X syndrome; and psychiatric ones such as schizophrenia and bipolar disorder. The initiative does not fund the collection of Alzheimer’s brains. Those are supported through the National Institute on Aging and the National Alzheimer’s Coordinating Center (see Part 3). However, member centers have archived AD material available and continue to accept AD brain donations using other funds.
Final Product.
Finished slides often include different stains on adjacent sections to support microscopic analysis of different aspects of pathology.
[Image courtesy of Netherlands Brain Bank.]
The NeuroBioBank encourages brain donations, particularly from people who died without a brain disease, and acts as a point of contact for potential donors. Public information is crucial for boosting the number of control brains in banks. “We need to engage the public and let them know this is an important endeavor,” Mash said. The Miami Brain Endowment Bank has done extensive outreach, and many healthy older people have participated in longitudinal studies through the bank and donated their brains for postmortem research, she added. One-third of the bank’s 2,000 brains came from people without a diagnosed illness.
The NIH project represents the broadest U.S. effort to collate brain tissue, but is not the only one. Taking a similar approach, the Autism BrainNet is developing its online portal, where researchers can access data associated with tissue donations.
Mash believes initiatives like these will advance the study of brain disorders by making brain tissue more readily available to researchers. “We honor the legacy of our brain donors by ensuring tissue is distributed widely to support the breakthroughs that will come,” she noted. —Madolyn Bowman Rogers
Brain Banks for Alzheimer’s, Parkinson’s Remain Underused
In the past decade, brain banks around the world have formed networks that set standards for handling and storing tissue, and combined data into inventories researchers can search for what they need (see Part 2 of this series, and Alzforum listing of consortia and brain banks). The Alzheimer’s field boasts one of the largest such networks of banked brains. The National Institute on Aging (NIA) in Bethesda, Maryland, currently supports 27 Alzheimer’s Disease Centers (ADCs), each of which has a neuropathology core. While the brains are stored locally, the ADCs have to submit all neuropathology, genetic, and clinical data to the National Alzheimer’s Coordinating Center in Seattle. The NACC database contains a wealth of associated longitudinal data on many thousands of samples, yet few researchers use this resource to the full, neurologists lamented to Alzforum. “I think the clinical and pathological data that comes out of the Alzheimer’s centers is superior to anything else,” said NIA’s Creighton (Tony) Phelps, who oversees the ADCs.
Pretty in Pink.
Hematoxylin and eosin stain highlights a fibrillar Aβ plaque in a frontal lobe section from an Alzheimer’s patient. [Image courtesy of Nigel Cairns, Washington University, St. Louis.]
How best to tap this resource? The NACC’s centralized database has an online query system that allows researchers to sort its contents by age, ethnicity, cognitive status, and ApoE genotype to find out which ADCs have brain samples that meet their study requirements. For researchers studying rare diseases such as corticobasal syndrome, or others who want to stratify samples by a genetic risk factor other than ApoE, NACC personnel will prepare a customized table of available tissue, said director Walter (Bud) Kukull. At the NIH Alzheimer’s Disease Research Summit last week in Bethesda, Maryland, Kukull urged the audience to make wider use of NACC, promising that its staff would respond to customized requests within a week.
Once researchers know where suitable samples reside, they request them from the local centers. All requests are granted, Kukull told Alzforum, although ADC personnel may ask scientists to modify their requirements to analyze fewer brains or look at a different brain region if the center cannot provide as much tissue as requested, especially for small areas in high demand, such as the hippocampus.
For most studies, researchers are better off obtaining all tissue from a single ADC, because each site processes and stores brains in a slightly different way, noted Peter Nelson, who directs the brain bank at the University of Kentucky ADC in Lexington. The standardization of BrainNetEurope and the NeuroBioBank (see Part 2) is not in place at the NACC. To mitigate this problem, in 2014 an NIA task force issued best practice guidelines to set minimum standards for brain banking at the ADCs. The guidelines stress the need to keep the postmortem interval short, quickly freeze tissue blocks or slices to avoid deterioration of RNA and DNA, and measure tissue integrity.
Alzheimer’s Hallmarks.
A modified Bielschowsky silver stain reveals a neuritic plaque (left) and neurofibrillary tau tangle (right).
[Image courtesy of Nigel Cairns, Washington University, St. Louis.]
However, the guidelines do not spell out exact methods, because neuropathologists like to do things their way, so samples vary somewhat between centers. All centers prepare both chemically fixed and frozen brain sections, as different experiments require different preparations. For example, studies of subcellular structures must be done in fixed, embedded sections, whereas extractions and biochemical experiments need frozen tissue. Often, pathologists fix half the brain for use in teaching and neuropathological diagnosis, and section the other half into thick coronal slices that are flash-frozen for later research use (Vonsattel et al., 2008).
An Abundance of Alzheimer’s Data
The major strengths of the NACC database are its size and the amount of information available on each donated brain, said Phelps. The NACC maintains data on more than 13,000 brains donated since 1984. The old samples come with minimal data, but since 2005, every brain donation caps extensive clinical and cognitive records from yearly assessments of the volunteer. About 3,000 brains belong to this Uniform Data Set (UDS). The number continues to grow, as around 30,000 patients are currently in treatment at ADCs nationwide, and about half of them have agreed to donate their brains upon death, Kukull said.
In the NACC database, nearly all donors had a memory disorder. Postmortem, about half of the UDS brains were diagnosed with AD, another 10 percent each with dementia with Lewy bodies (DLB), frontotemporal dementia, or AD pathology that did not reach the diagnostic threshold, and 6 percent with vascular dementia. A handful of donors had other conditions, such as hippocampal sclerosis or prion disease. Minorities are underrepresented in this sample, making up only 6 percent.
Control brains represent the greatest limitation of the NACC database. The ADC banks contain only about 140 brains without any evident pathology. Completely healthy brains are rare because almost all older people have some degree of pathology, such as modest tau deposits in the medial temporal lobe, said Nigel Cairns of the Knight Alzheimer’s Disease Research Center at Washington University in St. Louis. While pristine brains are in short supply, most banks contain a larger (though still insufficient) number of brains from cognitively healthy people who had minimal pathology. These serve as controls for most studies. “From a research point of view, that is not a problem,” Cairns said.
The UDS data that accompany each brain sample comprise clinical history, neurologic exams, neuropsychological test batteries, and functional rating scales, as well as the neuropathologic diagnosis. Most brain donations also include DNA and blood samples, which are stored in a central location at the National Cell Repository for Alzheimer’s Disease at Indiana University Medical Center in Indianapolis. The NACC currently does not collect biomarker data, but researchers can request that directly from the centers. A new version of the UDS starting later this year will incorporate biomarker data, Kukull said.
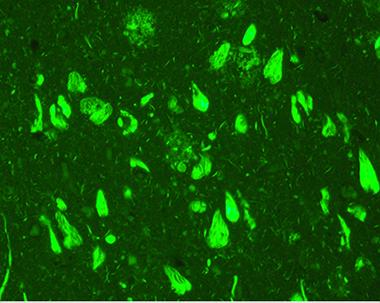
Amyloid Burden.
Thioflavin S stain lights up amyloid deposits that choke neurons and processes. [Image courtesy of Nigel Cairns, Washington University, St. Louis.]
“This highly annotated clinical and laboratory information greatly enhances the research value of a brain donation,” Thomas Montine, who directs the University of Washington ADC in Seattle, told Alzforum. Other researchers agree. “You can do amazing clinico-pathological correlations with NACC data,” Nelson said. This includes generating and testing hypotheses and analyzing genetic and environmental risk factors. “You may not even need to do a biochemical experiment, because there’s so much you can do with the data they already have on hand,” Nelson noted. As with tissue, researchers can request NACC data through an online query. NACC staff will prepare data reports, help with statistical analysis, discuss research questions, and even critique manuscripts before publication. “I think the asset is underutilized,” Nelson said.
Parkinson’s Field Builds Longitudinal Datasets
Researchers specializing in Parkinson’s disease have no such large resource as the NACC, but several smaller programs do store tissue. The Banner Sun Health Research Institute Brain and Body Donation Program in Sun City, Arizona, is a place to start, noted Beth-Anne Sieber at the National Institute of Neurological Disorders and Stroke. Like the ADCs, the program enrolls participants in a longitudinal clinical study, which at Banner includes brain and body donation at death (see Beach et al., 2008). The total collection contains more than 1,600 brains and 430 whole-body donations, which span the gamut from healthy controls to people diagnosed with Parkinson’s or Alzheimer’s disease (Beach et al., 2015). NINDS supports the PD portion of the Banner program, while NIA supports the AD portion.
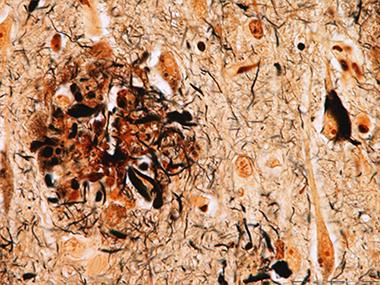
Deadly Dots?
Low- and high-resolution images of Marinesco bodies (purple-black) in the nuclei of dopaminergic cells in the substantia nigra. These neurons contain the natural pigment neuromelanin (brown).
[Image courtesy of Thomas Beach, Sun Health Research Institute, Sun City, Arizona.]
While the number of brains with Parkinson’s disease and related disorders just passed 200, each comes with extensive data, including DNA and blood samples. This enables researchers to perform sophisticated analyses, Sieber said. The tissue is of very high quality, as brains are processed within two hours after death, she added. Related disorders include DLB, Parkinson’s disease with dementia, multiple system atrophy, and progressive supranuclear palsy. Banner recently joined the Parkinson’s Disease Biomarkers Program, a new portal that will enable researchers to submit requests for biomarker data and associated tissue requests to the Banner brain bank, Sieber said. Having brain tissue from multiple similar disorders helps researchers parse the potential contributions of unusual pathologies such as Marinesco bodies, inclusions that appear in the nucleus of dopaminergic neurons and multiply with age (see image below). The spots occur more often in neurons that contain Lewy bodies, and correlate with a drop in key dopaminergic enzymes, hinting that they may contribute to the dysfunction of these cells (see Beach et al., 2004).
Another Option: Prospective Tissue Collection
The non-profit National Disease Research Interchange offers customized collection of brain tissue. NDRI was founded in 1980 by Lee Ducat, whose son had diabetes, when she realized researchers were having a bear of a time obtaining pancreas samples for research. The organization is based in Philadelphia and receives funding from the NIH as well as charitable donations. NDRI does not bank tissues; rather, it procures them prospectively for specific research studies. To use the service, researchers fill out an online application. NDRI scientists peer-review each application, and if they consider the study relevant and feasible, they help the researcher procure donated tissue, said Thomas Bell, who directs scientific services at NDRI. NDRI even becomes a consulting research partner, helping researchers with all stages of a project, from writing grants to preparing papers. “It normally turns into a long-term relationship. We have had scientists with us for 30 years,” Bell said.
To find the tissues, NDRI turns to a network of partners from hospitals to transplant organizations. These sites recover the tissue and prepare it according to the researcher’s specifications. The service would be particularly valuable for neuroscience researchers who need tissues prepared according to unusual specifications, or who want to analyze matched tissues, for example eye and visual cortex from the same donor, Bell noted. NDRI can prepare whole brains, or only a portion, such as the hippocampus. The timeline to fill requests varies from weeks to months to a year, depending on the rarity of the tissue. For example, if an Alzheimer’s researcher had numerous specific requirements regarding age, clinical status, and genotype of donors, it could take NDRI several weeks to obtain each brain. For many researchers this timeline works well, as it may take that long to perform experiments on each sample, Bell said. The service would be unsuitable for researchers who wanted to analyze samples from dozens of brains at the same time.
NDRI accepts brain donations from individuals. All donations include demographic and clinical data provided by the hospital and next of kin, which are then de-identified. NDRI has international clients and participates in large, multi-year projects. As with brain banks, researchers pay tissue-recovery, processing, and shipping costs.
Many resources are ostensibly only a few clicks away. Alas, in practice, neuroscientists are still hampered by the limited numbers of some kinds of brain, particularly from minorities, controls, and people with rare diseases. These problems are unlikely to be solved without a funding commitment that would enable brain banks to expand and reach out to the public for more participation. “Brain banking is a very expensive undertaking, and it’s never been well-funded,” noted Deborah Mash, who runs the University of Miami Brain Endowment Bank.—Madolyn Bowman Rogers
Beach TG, Adler CH, Sue LI, Serrano G, Shill HA, Walker DG, Lue L, Roher AE, Dugger BN, Maarouf C, Birdsill AC, Intorcia A, Saxon-Labelle M, Pullen J, Scroggins A, Filon J, Scott S, Hoffman B, Garcia A, Caviness JN, Hentz JG, Driver-Dunckley E, Jacobson SA, Davis KJ, Belden CM, Long KE, Malek-Ahmadi M, Powell JJ, Gale LD, Nicholson LR, Caselli RJ, Woodruff BK, Rapscak SZ, Ahern GL, Shi J, Burke AD, Reiman EM, Sabbagh MN.
Arizona Study of Aging and Neurodegenerative Disorders and Brain and Body Donation Program.
Neuropathology. 2015 Aug;35(4):354-89. Epub 2015 Jan 26
PubMed.








Comments
No Available Comments
Make a Comment
To make a comment you must login or register.