Cognitive Decline in Young Football Player Tied to Extensive Brain Damage
Quick Links
A growing number of former football players and other athletes have been diagnosed postmortem with the degenerative condition chronic traumatic encephalopathy (CTE). While these players had complained of cognitive problems and suffered deterioration in mood and behavior during life, none of them had had formal neuropsychological testing. Now researchers led by Ann McKee at Boston University have published the first case study that includes such testing. Appearing in the January 4 JAMA Neurology, the case involves a college football player who developed headaches, anxiety, and memory problems that led him to quit football and drop out of school. Neuropsychological testing found executive and learning deficits, but largely preserved episodic memory. The player died at age 25 of a heart attack after a staphylococcus infection inflamed his cardiac tissues. Postmortem examination revealed the most severe case of CTE yet seen in someone so young. It was similar to the degeneration found in players in their 40s, McKee noted.
“The data suggest there might be a neuropsychological profile for CTE individuals that would be different from an Alzheimer’s disease patient. If confirmed by other cases, this could serve as a biomarker of the disease,” suggested Robert Cantu at Boston University. He works with the authors but was not involved in this study.
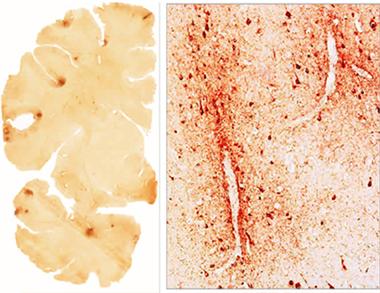
Early CTE.
Hubs of tau tangles (brown) dot the cortex of a 25-year-old former college football player. [Courtesy of Mez et al., ©2016 American Medical Association, all rights reserved.]
CTE has only been recognized in professional athletes in the last decade (see Jan 2007 news; Nov 2012 news series). Several large studies are now underway to find biomarkers for the condition (see Feb 2013 news; Dec 2015 news). McKee leads the Understanding Neurologic Injury and Traumatic Encephalopathy (UNITE) study, which correlates neuropathology with retrospective clinical and behavioral data to refine diagnostic criteria (see Mez et al., 2015).
The current case was part of the UNITE study. The young man played football from the age of six until 22. He had his first recognized concussion at the age of eight, and racked up at least 10 more over the years. After getting knocked out during his freshman year in college, he developed headaches, blurry vision, insomnia, and problems with concentration. His symptoms continued and progressed, even after he quit football in his junior year. After he dropped out of college, he became depressed and started abusing his wife. Neuropsychological testing a few months before his death detected impairments on executive tasks such as the Trail Making and Symbol Digit Modalities tests, language difficulties on the Boston Naming Test, and poor recall on the California Verbal Learning Test. At the same time, he tested as average intelligence, with intact reading ability and episodic and visual memory.
Based on his symptoms and test scores, the clinical panel unanimously diagnosed him with post-concussive syndrome, although they suggested CTE as a possible secondary contributing factor. Neuropathological examination later confirmed widespread CTE. McKee noted that it is still difficult for clinicians to distinguish this disorder during life.
CTE has been found in boys as young as 17, but those cases had limited, focal tau pathology, McKee said (see McKee et al., 2013). It is unclear why this college player developed such aggressive pathology, though it may have something to do with the early age at which he began playing. Cantu noted that several studies indicate that NFL players who started before the age of 12 perform worse on cognitive tests and have more impulse-control problems, depression, and anxiety than those who started playing at a later age. “We think the developing brain is more sensitive to traumatic injury and may experience greater effects,” McKee said.
In an accompanying JAMA Neurology editorial, James Noble at Columbia University, New York, wrote, “What stands out from this case is that 10 years after the first publication of CTE in football … a case report remains highly informative in framing important unmet needs in the field of concussion.” These include questions such as how often concussions actually occur in contact sports, what the lifetime risks of CTE are, and what puts some athletes at greater risk for degeneration than others with similar head injuries, Noble wrote. Researchers agree it will take long-term, large prospective studies to answer these questions.
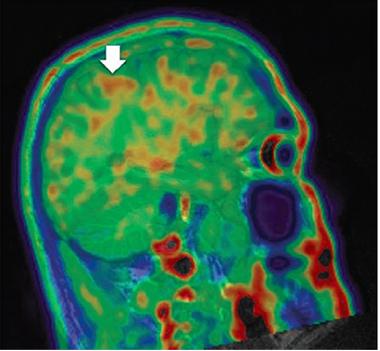
CTE in Progress.
Tau PET detects tangles (brown) in the cortex of a former football player with cognitive problems. [Courtesy of ADDF CTE Imaging Consortium, Curr Res Concussion.]
New biomarkers such as tau PET imaging may help shed light on these issues. In the December 31 Current Research: Concussion, researchers in the Alzheimer’s Drug Discovery Foundation CTE Imaging Consortium led by Dara Dickstein and Samuel Gandy at Icahn School of Medicine at Mount Sinai, New York, presented the first T807 tau image from a retired NFL player (see image at left). The subcortical pattern of tau accumulation matches the CTE signature determined by the NINDS Consensus Group, Gandy said (see McKee et al., 2016). He noted that this player, while symptomatic, is still highly functional. “[That] makes me optimistic about the prospects of T807 imaging for pre-symptomatic detection,” Gandy wrote to Alzforum (see full comment below). “At a minimum, with screening, we can get an idea of the prevalence of this tauopathy and perhaps begin to define the natural history.”—Madolyn Bowman Rogers
References
News Citations
- Butting Heads—Autopsies Fuel Debate on Football and Neurodegeneration
- Harvard Secures $100M to Study Brain Trauma, Other Football Injuries
- Large Grant for Chronic Traumatic Encephalopathy Biomarker Study
Conference Coverage Series Citations
Paper Citations
- Mez J, Solomon TM, Daneshvar DH, Murphy L, Kiernan PT, Montenigro PH, Kriegel J, Abdolmohammadi B, Fry B, Babcock KJ, Adams JW, Bourlas AP, Papadopoulos Z, McHale L, Ardaugh BM, Martin BR, Dixon D, Nowinski CJ, Chaisson C, Alvarez VE, Tripodis Y, Stein TD, Goldstein LE, Katz DI, Kowall NW, Cantu RC, Stern RA, McKee AC. Assessing clinicopathological correlation in chronic traumatic encephalopathy: rationale and methods for the UNITE study. Alzheimers Res Ther. 2015 Oct 12;7(1):62. PubMed.
- McKee AC, Stein TD, Nowinski CJ, Stern RA, Daneshvar DH, Alvarez VE, Lee HS, Hall G, Wojtowicz SM, Baugh CM, Riley DO, Kubilus CA, Cormier KA, Jacobs MA, Martin BR, Abraham CR, Ikezu T, Reichard RR, Wolozin BL, Budson AE, Goldstein LE, Kowall NW, Cantu RC. The spectrum of disease in chronic traumatic encephalopathy. Brain. 2013 Jan;136(Pt 1):43-64. PubMed.
- McKee AC, Cairns NJ, Dickson DW, Folkerth RD, Keene CD, Litvan I, Perl DP, Stein TD, Vonsattel JP, Stewart W, Tripodis Y, Crary JF, Bieniek KF, Dams-O'Connor K, Alvarez VE, Gordon WA, TBI/CTE group. The first NINDS/NIBIB consensus meeting to define neuropathological criteria for the diagnosis of chronic traumatic encephalopathy. Acta Neuropathol. 2016 Jan;131(1):75-86. Epub 2015 Dec 14 PubMed.
External Citations
Further Reading
Primary Papers
- Mez J, Solomon TM, Daneshvar DH, Stein TD, McKee AC. Pathologically Confirmed Chronic Traumatic Encephalopathy in a 25-Year-Old Former College Football Player. JAMA Neurol. 2016 Mar 1;73(3):353-5. PubMed.
- Noble JM. The Long Drive Ahead to Better Understanding Chronic Traumatic Encephalopathy: First (Case) and 10 (Years Later). JAMA Neurol. 2016 Mar 1;73(3):263-5. PubMed.
- ADDF CTE Imaging Consortium. Chronic traumatic encephalopathy: Diagnosing the repetitively injured brains of athletes and soldiers. Curr Res Concussion. 2015 Dec 31.
Annotate
To make an annotation you must Login or Register.
Comments
Icahn School of Medicine at Mount Sinai
The Mez et al. report is important in pointing toward the possible roles of youth, high school, and collegiate sports in the pathogenesis of CTE.
Also on CTE, we just reported the first image of T807 retention in a retired NFL player. It shows a subcortical pattern strikingly similar to the pattern of tauopathy that is the signature of CTE as recently reported by the NINDS consensus group (McKee et al., 2016).
A detailed case report on this retired NFL player will be presented by Dara Dickstein, Icahn School of Medicine at Mount Sinai, later this month at the Keystone meeting on CTE.
This patient has clinical CTE but is still highly functional, which makes me optimistic about the prospects of T807 imaging for pre-symptomatic detection. The challenge will be developing protocols for interacting with parents, coaches, school boards, colleges, and professional teams. At a minimum, with screening, we can get an idea of the prevalence of this tauopathy and perhaps begin to define the natural history.
I am not yet convinced of just how pervasive a problem we are facing. Tauopathy is not always clinically important and there are examples of reversible tauopathy (e.g., during hibernation). Still, I think that these images, when positive, might indicate who is at risk and should at least consider refraining from high-impact sports and careers.
References:
McKee AC, Cairns NJ, Dickson DW, Folkerth RD, Keene CD, Litvan I, Perl DP, Stein TD, Vonsattel JP, Stewart W, Tripodis Y, Crary JF, Bieniek KF, Dams-O'Connor K, Alvarez VE, Gordon WA, TBI/CTE group. The first NINDS/NIBIB consensus meeting to define neuropathological criteria for the diagnosis of chronic traumatic encephalopathy. Acta Neuropathol. 2016 Jan;131(1):75-86. Epub 2015 Dec 14 PubMed.
Quietmind Foundation
This report of extensive CTE in a young adult with repeated concussions is a cautionary tale. PET scanning of taupathy probably will not be adopted widely to detect CTE in adolescent athletes. However, diffusion tensor imaging of sports-related concussion has been reported in adolescents with concussion. It should be more readily available in community hospitals, as it has demonstrated structural changes in white matter after sports-related concussion. Then prevention, for example via an NIR helmet, might reduce CTE in adolescents and young adults with concussion.
References:
Virji-Babul N, Borich MR, Makan N, Moore T, Frew K, Emery CA, Boyd LA. Diffusion tensor imaging of sports-related concussion in adolescents. Pediatr Neurol. 2013 Jan;48(1):24-9. PubMed.
Nichols TW. Hyperphosphorylation of Tau Protein in Down’s Dementia and Alzheimer’s Disease: Methylation and Implications in Prevention and Therapy. J Alzheimers Dis Parkinsonism. 2014 Oct 6;(4):159.
Morries LD, Cassano P, Henderson TA. Treatments for traumatic brain injury with emphasis on transcranial near-infrared laser phototherapy. Neuropsychiatr Dis Treat. 2015;11:2159-75. Epub 2015 Aug 20 PubMed.
Make a Comment
To make a comment you must login or register.